AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-4861/036
1 Division of Infectious Disease, Department of Internal Medicine, Brody School of Medicine at East Carolina University, Greenville, NC.
2 Department of Public Health at East Carolina University, Greenville, NC.
3 Department of Internal Medicine Brody School of Medicine at East Carolina University, Greenville, NC.
4 Division of Infectious Diseases, Department of Internal Medicine, University of Wisconsin, Madison, WI.
*Corresponding Author: Dora Lebron, MD 2390 Hemby Lane Greenville, NC 27834, Division of Infectious Disease, Department of Internal Medicine, Brody School of Medicine at East Carolina University, Greenville, NC.
Citation: Dora L, Alexandra S, Alicia L, Rabindra G, Marysia G, et all. (2020) Sustained Virologic Response Rates of Direct Acting Antivirals in HIV Coinfected Hepatitis C Patients and Its Effect on Liver Fibrosis. International Journal of Clinical Case Reports and Reviews, 3(2); DOI:10.31579/2690-4861/036
Copyright: © 2020 Dora Lebron, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 July 2020 | Accepted: 26 August 2020 | Published: 31 August 2020
Keywords: direct acting antivirals; fibrosure™; hepatitis c virus; human immunodeficiency virus; metavir; sustained virologic response
Background: Hepatitis C virus (HCV) is an important cause of chronic hepatitis with necroinflammation and fibrosis resulting in end stage liver disease and hepatocellular carcinoma. Direct acting antivirals (DAAs) are newer agents that directly interfere with the HCV lifecycle and result in high rates of sustained virologic response (SVR). We evaluated if treatment with DAAs in a real-world setting is as successful in HCV/HIV coinfected patients as it is in HCV monoinfected patients, and if some degree of fibrosis regression can be observed after completion of therapy in both groups.
Methods: We retrospectively reviewed data from HCV monoinfected and HCV/HIV coinfected patients who received treatment from 2014-2016 at the East Carolina University Infectious Diseases clinic. The primary outcome was to compare completion and sustained virologic response (SVR) rate at either 12 or 24 weeks between HCV monoinfected patients and HCV/HIV coinfected patients. The secondary outcome was to assess regression of fibrosis at either 12 or 24 weeks after completion of therapy, defined as one METAVIR stage improvement in their FibroSure™, a noninvasive biochemical test to estimate the stage of fibrosis.
Results: There were 41 patients in each group. Compared to the coinfected group, patient no show rate was higher in the monoinfected group (p=0.0346). In the HCV monoinfected group, 25 (93%) achieved either SVR 12 or 24. Two patients were non-compliant and had detectable viral load on evaluation at week 12. In the HCV/HIV coinfected group, 37 patients achieved SVR (p=0.0039). One patient in the coinfected group did not complete therapy but achieved SVR. In terms of fibrosis, 12/18 (67%) in the monoinfected group demonstrated improvement in at least 1 Metavir stage and 6/18 (33%) had no change. In the coinfected group, 8/16 (50%) patients demonstrated an improvement in FibroSure™ stage, 5/16 (31%) had no change, and 3/16 (19%) had worsening fibrosis according to FibroSure™ stage, (p=0.4867).
Conclusions: In this small, real-world cohort, HCV/HIV coinfected patients treated with DAAs had higher completion and SVR rates than HCV monoinfected patients. Treatment failures in the monoinfected group were all linked to non-adherence, whereas, more coinfected patients achieved SVR, likely related to the fact that they were regularly engaged in routine HIV care. Fibrosis regression based on FibroSure™ was observed more in monoinfected patients than those with coinfection. Although not statistically significant, at least 50% of the patients in each group had regression of fibrosis.
Hepatitis C virus (HCV) is a blood-borne virus that can cause chronic hepatitis. Approximately 15-45% of infected persons spontaneously clear the virus within 6 months.[1] People unable to clear the infection develop chronic hepatitis, characterized by necroinflammation accompanied by a variable degree of fibrosis, end stage liver disease, and hepatocellular carcinoma (HCC). It is estimated that 150 million people around the world have chronic HCV and the risk of developing cirrhosis in 20 years is around 15-30%.[2] Chronic hepatitis C infection has been associated with mixed cryoglobulinemia, cryoglobulinemic vasculitis, B-cell non Hodgkin lymphoma, SICCA syndrome, polyarteritis nodosa, monoclonal gammopathies, and immune thrombocytopenia. [3,4,5] Around 85% of patients with HCV will become chronically infected developing long-term complications associated with cirrhosis and extrahepatic manifestations representing a high economic burden.[6] In the United States, approximately 10% of the patients with Hepatitis C are coinfected with human immunodeficiency virus (HIV). HIV coinfected individuals are less likely to spontaneously clear the infection due to an impaired T cell response to HCV and are at higher risk to progress to cirrhosis with HIV viremia. This rapid progression may be attributable to weaker immune response against HCV, the effect of HIV on hepatic cells, and amplified microbial translocation accelerating fibrosis. [7, 8, 9] With the introduction of the direct acting antivirals (DAAs), a new era of hepatitis C treatment has emerged. Unlike interferon, DAAs interfere with various steps of the HCV lifecycle, similar to the way antiretroviral drugs work against HIV. [10] In HCV/HIV coinfected patients, treatment with pegylated-interferon based therapy was associated with lower sustained virologic response (SVR) rates, higher rate of adverse effects and drug-drug interactions when compared to monoinfected patients. [11, 12, 13] In this small real- world cohort, we compared treatment response in HCV monoinfected patients and HCV/HIV coinfected patients.
Changes in fibrosis after completion of therapy using the FibroSureTM stages were also evaluated in both groups.
Methods Study Design
In this retrospective study, we reviewed the medical records of 82 HCV monoinfected and HCV/ HIV coinfected patients presenting at East Carolina University Infectious Disease Clinic from January 2014 through December 2016. All patients were either treatment-naïve or treatment- experienced with interferon +/- ribavirin and at least 18 years of age. The Institutional Review Board approved all aspects of this study. Data collected included demographics (age, sex, and race), HIV status, and HCV genotypes. Laboratory values abstracted included alanine aminotransferase (ALT), platelet count, HCV ribonucleic acid (HCV RNA) at 4 weeks and 12 weeks of treatment, also at 12 or 24 weeks after completion of therapy. Among HIV-infected patients, CD4 and HIV viral load were measured. Treatment modalities, including type of DAA therapy and antiretroviral (ART) regimens were documented. Alcohol abstinence was a requirement to qualify for treatment.
The primary outcome was to compare completion rate and sustained virologic response at either 12 (SVR12) or 24 (SVR24) weeks after completion of therapy between HCV monoinfected and HCV/ HIV coinfected patients. The secondary outcome was to evaluate fibrosis regression and compare it between both groups using HCV FibroSureTM assay. This is a noninvasive biochemical test that measures liver fibrosis activity. The FibroSureTM results correspond to the METAVIR scoring system for stage of fibrosis. It is based on a 5-point scale from 0 to 4 for the stage of liver fibrosis. METAVIR classifications recorded were F0, no fibrosis/ F1, portal fibrosis without septa/ F2, portal fibrosis with few septa/ F3, numerous septa without cirrhosis/ F4, cirrhosis. Baseline fibrosis was determined and dichotomized (<F2 for mild fibrosis and >F3 for advanced fibrosis). FibroSureTM was obtained at baseline and either 12 or 24 weeks following treatment. Improvement in fibrosis was defined as one METAVIR stage improvement in FibroSureTM from baseline to 12 or 24 weeks after completion of therapy (FibroSureTM stage at baseline (FB) - FibroSureTM stage at SVR12 or 24 (FSVR) = delta (Δ) FibroSureTM stage). Changes in fibrosis were defined as: (Δ) FibroSureTM stage <0 - worsening fibrosis, (Δ) FibroSureTM stage =0-0.5 - no change and (Δ) FibroSureTM stage >1 - improvement).
Statistical Analysis
Chi square test and Fisher’s Exact Test were used for categorical variables and to determine statistical significance between HCV monoinfected and HCV/HIV coinfected groups for completion of treatment, SVR 12 or 24, and changes in fibrosis. Student t-test was used for continuous variables. For all statistical analyses, a 0.05 level of significance was used, and all p- values were two-sided. Statistical analysis was performed using GraphPad Prism, version 7.0d.
Results
Study Population
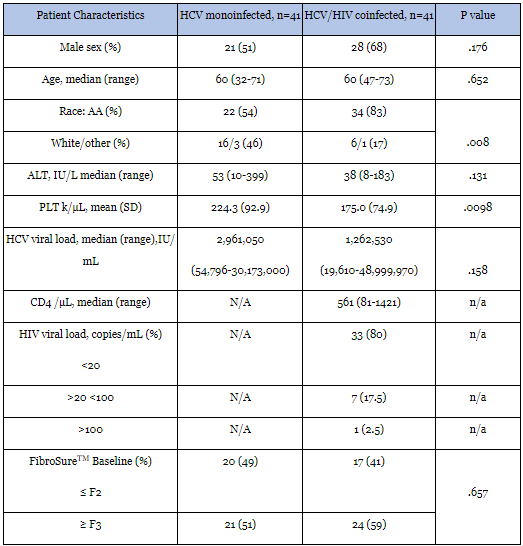
We identified 82 HCV infected patients, 50% (n=41) of which were coinfected with HIV (Figure 1). The overall median age was 60 years (Range, 32-73). Majority of the patients were African- American (68.3%), and male (59.5%). While age was not different by sex, it was different by race: African-Americans were, on average, 60.2 years (SD, 6.4), whites, 54 years (SD, 7.1), and other, 57 years (SD, 8.3), p<.0001.
HCV Monoinfected versus HCV/HIV Coinfected Patients
As seen in Table 1, the median HCV viral load in the monoinfected group was 2,961,050 IU/mL (range: 54,796-30,173,000) compared to the median HCV viral load in coinfected group that was 1,868,300 IU/mL with a range 19,610-48,999,970 (p=0.158). In the HCV/HIV coinfected group, most patients were virally suppressed with 97.5% of the patients with a viral load <100 copies/ mL and 1 patient with 370 copies/mL. Median CD4 count was 561 k/µL with a range (81-1421). Only 2 patients had CD4 <200 and both had undetectable HCV viral load at completion of therapy.
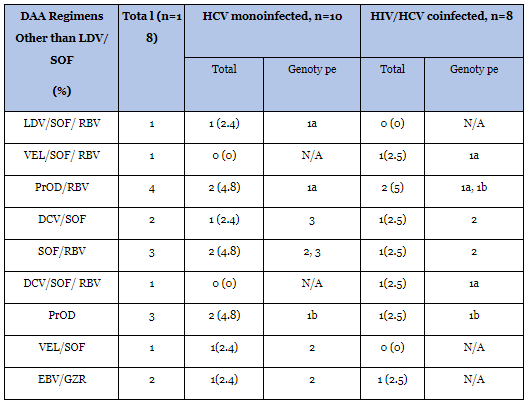
FibroSure TM results were divided as < F2 for mild fibrosis and > F3 for advanced fibrosis. In the monoinfected group, 49% had mild fibrosis and 51% had advanced fibrosis at baseline. Meanwhile, in the coinfected group, 41% had mild fibrosis and a higher percentage, 59% had advanced fibrosis (p=0.657). Regarding DAA regimens, 78% of the patients were treated with ledipasvir/sofosbuvir (see Table 2) as 67% of the patients had genotype 1a. Twelve percent of the patients in the monoinfected group were treatment experienced vs 15% in the coinfected group.
SVR in HCV Monoinfected versus HCV/HIV Coinfected Patients
From the 41 patients in the monoinfected group, data was collected from 27 patients (see Figure 1). Fourteen patients were not evaluated for SVR 12 or 24 as they lost follow up, but 13/14 patients were undetectable at either 4, 8 or 12 weeks of treatment. From the 27 patients that followed up, 25 (93%) achieved either SVR 12 or 24. Two patients (7%) had detectable viral load at completion of therapy. In the HIV/HCV coinfected group, data was obtained from 37 patients, 4 patients lost follow up. One patient did not complete therapy but continued follow up. The 4 patients that lost follow up had undetectable viral load at either 4, 8 or 12 weeks of treatment. The coinfected patient that did not complete therapy had a HCV viral load of 252,590 IU/mL and achieved SVR after receiving 4 weeks of therapy. All 37 (100%) patients in the coinfected group that followed up had documented SVR 12 or 24.
Changes in Fibrosis in HCV Monoinfected versus HCV/HIV Coinfected
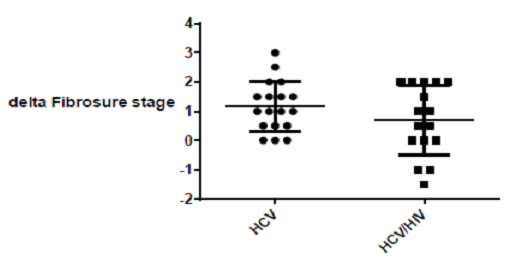
In terms of fibrosis in the monoinfected group, FibroSureTM after SVR either at 12 or 24 weeks was collected from 18 patients. Twelve patients (67%) demonstrated improvement in at least one METAVIR stage in FibroSureTM and 6 (33%) had no changes in FibroSureTM. Worsening of fibrosis was not observed in the monoinfected group at either SVR 12 or 24 weeks. In the HIV/HCV coinfected group, FibroSureTM at either 12 or 24 weeks of completion of therapy was obtained in 16 patients. Eight patients (50%) demonstrated improvement of fibrosis, 5 (31%) had no changes in FibroSureTM stage and 3 (19%) had worsening of fibrosis according to FibroSureTM stage (See Figure 2). The three patients that had worsening fibrosis were African-American, males, 58 years or older with CD4 count above 350/µL, 2 of them had HIV undetectable viral load, and 1 had 350 copies/mL. HCV viral load in these 3 patients ranged from 2,743,110 - 5,294,540 IU/mL, and antiretroviral (ARV) regimen consisted of an integrase inhibitor (INSTI) and 2 nucleoside reverse transcriptase inhibitors (NRTIs).


This small cohort provides real world data about the efficacy of DAAs in HCV monoinfected, but more importantly, in HCV/HIV coinfected patients. In previous clinical trials where HCV monoinfected patients were treated with interferon-based and ribavirin therapy, SVR rates ranged from 35% to 50% in genotypes 1 or 4, and up to 80% in genotypes 2 or 3. [14, 15] These regimens were associated with increased costs, poor tolerability, and adverse effects. [11, 12] In HCV/HIV coinfected patients, poorer responses were documented and higher rates of adverse effects were observed. [16,19] Not only low SVR rates, but also progression of HCV-related liver damage including fibrosis became a major area of concern, especially in the era prior to DAAs. Factors that contribute to worsening prognosis besides HIV seropositivity include alcohol consumption, older age at the time of HCV infection, and CD4 count < 200 cells/mm3, which are also associated with a higher rate of fibrosis progression. [20,22]
In this study, HCV/HIV coinfected patients treated with DAAs demonstrated higher SVR rates than HCV monoinfected patients with overall well tolerability. Our study correlates with multiple other studies where coinfected patients, in real world setting achieved high SVR rates. Del Bello, et al published data with sofosbuvir containing regimens in which coinfected patients achieved high SVR rates with minimal adverse effects. SVR rates in coinfected patients did not vary with ARV regimen used. [23] In ALLY-2 study, SVR 12 was achieved in 97% or more patients receiving any ARV regimen. [24] The ION 4 study with coinfected patients documented high rates of sustained virologic response that ranged from 96 to 100%. [25] In the PHOTON-1 trial, 67-88% of treatment-naive participants achieved SVR12, while among treatment-experienced participants, 92-94% achieved SVR12. [26] In our study, 11 patients were treatment experienced, and all of them achieved SVR at 12 or 24 independently of HIV coinfection.
More patients in the monoinfected group did not attend all of the scheduled appointments as compared with the coinfected group. In the HCV monoinfected group, 25 (93%) achieved either SVR 12 or 24. Two patients were non-compliant and had detectable viral load on evaluation at week 12. In the HCV/HIV coinfected group, 37 patients achieved SVR, while interestingly one patient in the HCV/HIV coinfected group received only 4 weeks of therapy but had undetectable viral load 4 weeks and remained undetectable to date.
Other studies have shown different results due to poor compliance in HIV coinfected patients. Lakshmi et al concluded that real world HCV cure rates with DAAs in HCV/HIV coinfection were lower than those seen in clinical trials. In their patients, cure was associated with attendance to follow up clinic visits and use of an integrase inhibitor based HIV regimen. Cure was achieved in 83.3%. [27] In our study, more HCV/HIV coinfected patients completed therapy and followed up (88% vs. 66%, respectively) and achieved SVR rates compared to monoinfected patients (88% vs 61%). We feel that this phenomenon is due to coinfected patients being already engaged in HIV care through Ryan White Program.
Before DAAs era, African-Americans had poorer response rates to pegylated interferon and ribavirin compared to Caucasians (28% vs 52%, respectively). [28,30] For this reason, AA patients with HCV/HIV coinfection were associated with a lower likelihood of receiving treatment for HCV. [31] In our clinic population, the AA population with HCV/HIV coinfection comprises a higher number than Caucasians. Compared to the monoinfected group, the coinfected population was composed of more AAs. In terms of ARV therapy, an INSTI with NRTI backbone was the most common regimen used due to safety and less drug-drug interactions (see Appendix Tables 3 and 4).


As SVR is considered the first step in decreasing morbidity and mortality in HCV infected individuals, assessment and monitoring of fibrosis after achieving SVR is an interesting field of investigation. It is known that HIV enhances liver damage progression and worsening fibrosis with more aggressive course of liver disease in coinfected patients. As DAAs have only recently become available, there is not enough data about the effects of SVR on liver fibrosis years after treatmenst. In a study on changes in fibrosis, Martinez et al compared liver fibrosis before and after antiviral therapy by different serum marker panels in patients with chronic hepatitis C using the Enhanced Liver Fibrosis (ELF) score. In the study, the ELF score decreased significantly in patients with SVR but remained unchanged in non-responders. A decrease in ELF score after antiviral treatment reflects the impact of viral clearance in hepatic extracellular matrix and probably in the improvement of liver fibrosis. [32]
Another study evaluated ELF scores and FibroScan® in 32 HCV-infected patients in Germany treated with SOF (93.8% SVR12). The study found biochemical response within 4 weeks and significant decrease from baseline to 12-week post-treatment follow-up in ELF and FibroScan® measurements, indicating improvement of the dynamics of liver fibrosis. [33] In our study, at SVR 12 or 24 weeks, at least 50% of patients in both groups demonstrated improvement in liver fibrosis defined as one Metavir stage improvement based on FibroSureTM stages. More patients in the monoinfected group demonstrated improvement in fibrosis although not statistically significant. There was no worsening fibrosis in the monoinfected patients compared to a 19% in the coinfected group possibly due to the effect of HIV on liver fibrosis despite viral suppression or antiretroviral therapy. Two of the coinfected patients with worsening fibrosis had undetectable HIV viral load, while the patient that had 1.5 worsening fibrosis, had 370 copies/mL. This is consistent with a study that showed accelerated fibrosis in HIV coinfected patients even if HIV replication is under control by ARVs. [8] As newer and better DAAs become available, and more data on SVR and liver fibrosis becomes available, further studies with larger sample size would be needed to study long-term effects of SVR on liver fibrosis in this population.
Our study has many limitations. Small sample size could skew the results that we have demonstrated here in larger studies. Use of certain hepatotoxic substances including over the counter medications, routine medications and alcohol could contribute to worsening of fibrosis, but we were unable to take these into account. We did not routinely obtain serum alcohol levels to know if participants used alcohol regularly. FibroSureTM as a biomarker has its limitations when compared to elastography or biopsy for the assessment of fibrosis. As assessment of fibrosis after HCV treatment is not part of the American Association for the Study of Liver Disease (ASSLD) guidelines, not all patients had the opportunity to obtain a FibroSureTM at 12 or 24 weeks after completion of therapy due to limited economic resources.
Conflict of interest:
Dora Lebron, MD – none
Manal Elnabtity, PharmD - none
Alexandra Stang, MD – none
Ahmed Hamed, MD - none
Alicia Lagasca, MD – none
Marysia Grzybowski - none
Rabindra Ghimire, MD – none
Dawd Siraj, MD – not known
Paul Cook, MD - PI for Gilead, Affinergy, Leonard-Meron Biosciences No financial support
Authors Contribution:
Dora Lebron – corresponding author
Manal Elnabtity - data curation
Alexandra Stang – data curation
Ahmed Hamed - data curation
Alicia Lagasca – supervising
Marysia Grzybowski - statistics
Rabindra Ghimire – supervising, editing
Dawd Siraj - supervising
Paul Cook – supervising, editing
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
